Private Label, White Label, Wholesale partnerships available - EU, USA and UK - Free shipping from €75
Differences in Sterile Solutions: A Clinical Reference Guide
Discover the crucial differences in sterile solutions. This guide helps clinicians and researchers make informed choices for safety and efficacy.
TL;DR:
- Different sterile solutions vary significantly in composition, endotoxin levels, and clinical suitability, impacting safety and outcomes. Proper selection based on application and rigorous quality controls, including endotoxin testing, are essential for laboratory and clinical use. Awareness of these distinctions helps prevent patient harm and research errors caused by solution misclassification or mishandling.
Not all sterile solutions are created equal, and the differences in sterile solutions go far beyond microbial cleanliness. Researchers and clinicians who treat sterile water, saline, bacteriostatic water, and pharmaceutical-grade WFI as interchangeable are exposing workflows, patients, and research outcomes to real risk. Composition, tonicity, endotoxin load, and regulatory grade each determine whether a solution is safe and fit for a specific application. This guide breaks down every critical distinction so you can make precise, well-informed decisions for laboratory and clinical use.
Table of Contents
- Key Takeaways
- Differences in sterile solutions: types and classifications
- Comparing key properties of sterile solutions
- Clinical and laboratory application differences
- Quality assurance and regulatory considerations
- My perspective on sterile solution selection in practice
- Quality sterile solutions for research and clinical use
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Sterile does not mean endotoxin-free | A solution can be microbiologically sterile yet still trigger pyrogenic reactions if endotoxin is not specifically controlled. |
| WFI meets the strictest standards | Water for Injection must not exceed 0.25 EU/mL endotoxin and 10 CFU/100 mL, making it the highest-grade option for injectable applications. |
| Tonicity drives clinical selection | Sterile saline is isotonic and preferred for wound care and infusion, while sterile water is hypotonic and carries hemolysis risk if used incorrectly. |
| Bacteriostatic water has specific limits | Benzalkonium chloride or benzyl alcohol in bacteriostatic water makes it unsuitable for neonates and certain injectable preparations. |
| Application must match solution grade | Using Purified Water where WFI is required, or saline where sterile water is needed, can compromise results or cause patient harm. |
Differences in sterile solutions: types and classifications
Before comparing properties, you need a solid map of the category. “Sterile solution” is a broad label covering several distinct product classes, each manufactured to different specifications.
Sterile water for injection (SWFI) is water that has been purified, sterilized, and packaged in a way that meets USP or pharmacopeial standards for injection use. It contains no added solutes, no antimicrobial agents, and no buffers. Because it is hypotonic, direct large-volume intravenous infusion without admixture is contraindicated.
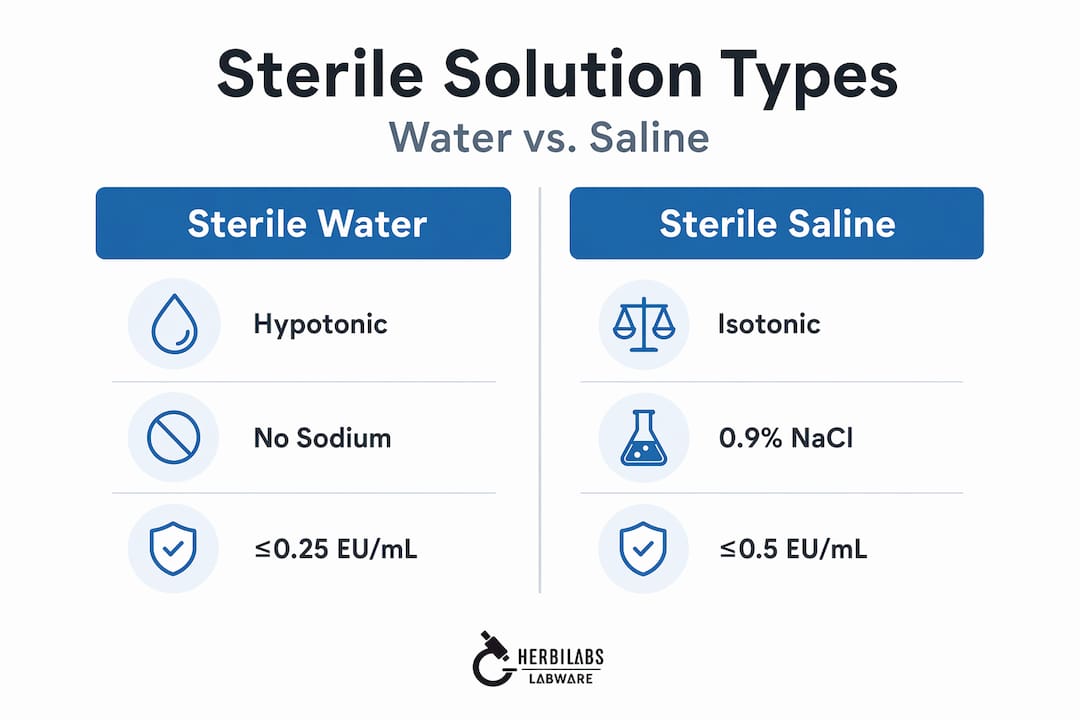
Sterile saline (0.9% NaCl) is an isotonic solution that matches plasma osmolality and is the most widely used clinical fluid for wound irrigation, inhalation therapy, and IV fluid resuscitation. The 0.9% sodium chloride concentration is the defining compositional feature, and it is what makes saline physiologically compatible in ways that plain sterile water is not.
Bacteriostatic water contains a preservative, most commonly benzyl alcohol at 0.9% or benzalkonium chloride, which inhibits microbial growth and permits multi-dose vial use. It is manufactured as a sterile product but is intended for reconstituting injectable medications across multiple draws from a single container. Understanding how bacteriostatic water differs from plain sterile water is foundational for any researcher working with peptide or protein reconstitution.
At the pharmaceutical water end of the spectrum, two grades dominate:
- Purified Water (USP): Used in laboratory reagent preparation, equipment rinsing, and non-injectable pharmaceutical manufacturing. Microbial limit is ≤100 CFU/mL with no endotoxin requirement.
- Water for Injection (WFI): Required for all parenteral preparations. Produced by distillation or validated membrane-based systems. Subject to strict endotoxin and conductivity controls.
The no endotoxin requirement for Purified Water versus the tightly controlled WFI specification is one of the most clinically significant distinctions in the entire category, and it is frequently misunderstood.
Comparing key properties of sterile solutions
Understanding how sterile solutions are different means going deeper than a product label. The properties that matter most are chemical composition, tonicity, microbial limits, and endotoxin control.
Chemical composition
The table below summarizes the core parameters across the major sterile solution types.
| Solution | Key components | Tonicity | Endotoxin limit | Microbial limit |
|---|---|---|---|---|
| Sterile water for injection | Water only, no additives | Hypotonic | ≤0.25 EU/mL | ≤10 CFU/100 mL |
| Normal saline (0.9% NaCl) | Water + 0.9% sodium chloride | Isotonic | ≤0.25 EU/mL (IV grade) | ≤10 CFU/100 mL |
| Bacteriostatic water | Water + preservative (BnOH or BAC) | Slightly hypotonic | Controlled | ≤10 CFU/100 mL |
| Purified Water (USP) | Highly purified water, no additives | Hypotonic | No requirement | ≤100 CFU/mL |
| Water for Injection (WFI) | Ultra-purified water | Hypotonic | ≤0.25 EU/mL | ≤10 CFU/100 mL |
Tonicity and its physiological implications
Tonicity is not a technicality. When you administer a hypotonic solution directly into vasculature, water moves into red blood cells by osmosis, causing them to swell and lyse. This is why sterile water for injection should never be infused in large volumes without admixture. Normal saline avoids this problem by matching the osmolality of plasma, making it the correct choice for isotonic expansion of extracellular volume.
Endotoxin and microbial standards
WFI must meet ≤0.25 EU/mL endotoxin alongside a microbial count of ≤10 CFU/100 mL. Purified Water is held to ≤100 CFU/mL with no endotoxin requirement at all. That gap matters enormously in practice. A batch of Purified Water can be completely free of viable organisms yet still carry enough endotoxin to trigger a serious pyrogenic reaction in a patient receiving a parenteral preparation made with it.

Endotoxins are heat-stable pyrogens that survive many standard sterilization processes. A solution can pass a sterility test and still fail on endotoxin. This is precisely why WFI specifications exist as a separate, more demanding category.
Pro Tip: When validating a new sterile solution for injectable or ophthalmic research applications, always request both sterility test results and limulus amebocyte lysate (LAL) endotoxin data from your supplier. A certificate of sterility alone does not tell the full story.
Clinical and laboratory application differences
Sterile solution composition only makes sense in the context of what the solution is actually supposed to do. The selection of correct sterile solutions for specific applications is where knowledge of property differences translates directly into safety outcomes.
Wound irrigation and topical use
Sterile saline is the preferred irrigant for wound cleaning across surgical and emergency care settings because its isotonicity minimizes tissue irritation. Sterile irrigation solutions are categorically distinct from IV fluids. They are applied externally to physically remove debris and pathogens, and they are never injected. Using sterile water for wound irrigation instead of saline is not necessarily harmful in small volumes, but the hypotonic exposure adds no benefit and can cause localized cellular stress in large lavage procedures.
Inhalation therapy
Nebulized medications require an isotonic carrier to avoid bronchospasm. Sterile saline serves this role. Using sterile water in a nebulizer would deliver hypotonic particulates into the airways, which can cause airway irritation, particularly in patients with reactive airways. This is a meaningful clinical distinction, not a minor formulation preference.
Equipment use: a common error
Sterile saline should not be used in CPAP machine humidifier chambers. Salt residue from repeated use damages internal components and can promote mineral buildup in the delivery pathway. Plain sterile or distilled water is the correct choice here. The isotonicity that makes saline ideal for vascular and wound applications becomes a liability in equipment maintenance.
Bacteriostatic water in research and clinical practice
Bacteriostatic water is the standard diluent for multi-dose peptide and protein reconstitution in laboratory and research settings. Its preservative content extends the usable life of a reconstituted vial by preventing microbial proliferation between draws. However, it carries specific contraindications. It should not be used in neonates, and it is unsuitable for intrathecal, epidural, or high-volume IV use. For a detailed breakdown of its research applications, bacteriostatic water uses in laboratory workflows are covered extensively in Herbilabs’ dedicated guide.
Pro Tip: Label every reconstituted vial with the solution type, concentration, date, and initials. Bacteriostatic water and sterile water for injection look identical. Confusing them in a multi-user lab environment is a documented source of reconstitution errors.
Quality assurance and regulatory considerations
Even when the right solution is selected, improper handling or inadequate quality controls can negate the benefits of that selection entirely.
-
Endotoxin testing at every production stage. Endotoxin control requires validated removal methods and routine sampling throughout the production and distribution chain. Point-of-use testing alone is not sufficient for high-risk parenteral applications.
-
Validated production systems for WFI. FDA now permits membrane-based WFI systems in addition to traditional distillation, provided they undergo full validation. Any WFI system must demonstrate consistent performance across conductivity, total organic carbon (TOC), microbial counts, and endotoxin limits.
-
Conductivity and TOC monitoring for Purified Water. These two parameters catch ionic and organic impurities that microbial testing misses entirely. A water system can produce sterile output that still fails on TOC if organic contaminants from tubing, filters, or reagents leach into the stream.
-
Sterile field maintenance in clinical workflows. Handling best practices require trained personnel, validated environmental controls, and aseptic technique at every point from product receipt through administration. A pharmaceutical-grade solution is only as good as the handling chain that delivers it to the point of use.
-
Shelf-life and container integrity. Single-dose sterile products have no preservative and must be used immediately after opening. Multi-dose bacteriostatic products have defined in-use stability periods that must be tracked and respected.
My perspective on sterile solution selection in practice
I’ve worked closely enough with pharmaceutical-grade water specifications to say this plainly: the most common and dangerous mistake I see is treating sterility as a binary pass/fail without asking what else the solution might be carrying. A product can clear every microbial test on the sheet and still contain enough endotoxin to cause a febrile reaction. Sterility and pyrogenicity are not the same thing, and laboratories that conflate them create blind spots in their safety protocols.
The labeling confusion problem is underappreciated. I’ve seen bacteriostatic water and sterile water for injection stored side-by-side with near-identical labeling from different suppliers. In a fast-paced research environment, that ambiguity gets people into trouble. My recommendation is to enforce a physical separation protocol in storage, not just a labeling system.
The other thing I’d push back on: the idea that pharmaceutical water grades are only a concern for large manufacturing operations. Any researcher reconstituting compounds for injectable use needs to apply the same scrutiny to their diluent that a pharmaceutical manufacturer would. The batch size doesn’t change the biology of endotoxin exposure. Selecting the right grade from a supplier with documented quality controls is not optional rigor. It is the baseline.
— Ragnar
Quality sterile solutions for research and clinical use
Herbilabs manufactures bacteriostatic water and sterile diluents to research-grade standards with documented endotoxin and microbial controls, specifically for the peptide research community across the UK and Europe. Every product is produced in a dedicated facility under strict quality protocols, so researchers receive consistent, contaminant-free solutions that meet the demands of injectable applications.
Whether you need multi-dose bacteriostatic water for reconstitution work or want to understand how different sterile diluents compare for your specific protocol, Herbilabs provides the product documentation and technical transparency to support informed decisions. Browse the bacteriostatic water FAQ for detailed answers on reconstitution standards, storage requirements, and application-specific guidance from professionals who supply to research institutions across Europe. Wholesale pricing and secure ordering are available for institutional and reseller customers.
FAQ
What is the main difference between sterile water and sterile saline?
Sterile water contains no solutes and is hypotonic, while sterile saline contains 0.9% sodium chloride and is isotonic. The tonicity difference determines their clinical applications: saline is preferred for wound irrigation and IV use because it matches plasma osmolality.
Why does WFI have stricter limits than Purified Water?
WFI is required for parenteral preparations where endotoxins enter the bloodstream directly, so it must meet ≤0.25 EU/mL endotoxin and ≤10 CFU/100 mL microbial limits. Purified Water allows up to ≤100 CFU/mL and has no endotoxin requirement because it is used in non-injectable applications.
Can bacteriostatic water be used for all injectable preparations?
No. Bacteriostatic water is contraindicated in neonates, and should not be used for intrathecal, epidural, or large-volume intravenous preparations. Its preservative content makes it appropriate for multi-dose reconstitution in research and certain clinical contexts only.
What does endotoxin testing actually tell you?
Endotoxin testing measures the presence of bacterial lipopolysaccharides that survive sterilization and cause pyrogenic reactions. A solution that passes sterility testing can still fail on endotoxin, which is why injectable-grade solutions require separate, validated endotoxin controls beyond standard microbial testing.
Is sterile saline safe to use in all medical equipment?
No. Sterile saline is unsuitable for CPAP humidifier chambers because the salt content causes mineral buildup and equipment damage over time. Plain sterile or distilled water is the correct choice for devices where ionic residue is a concern.


